")





A new concept of the physiopathology of the venous circulation in the lower limbs clearly demonstrates that varicose veins must not be removed, obliterated, ligated or burnt; they must simply be regenerated along with the dilated and dilatable veins of the perforating and communicating circulation (regeneration = restoration of the form and function).
Sclerotherapy, phlebectomy, saphenectomy, laser therapy, high-frequency currents and functional ligature act only on the effect of the pathology, not on its cause. These approaches act on sporadic dilated veins, while ignoring the fact that the objective of the treatment of varicose disease is to eliminate the hemodynamic hypertension in the superficial and perforating venous circulation.
Indeed, obliterating or removing superficial dilated veins, as the traditional methods do, means eliminating the escape valves for the hypertension that these traditional techniques are unable to treat. Removing or obliterating these escape valves merely generates further varicose veins and telangiectasias. If we insist on removing or obliterating the veins of the superficial circulation, these dilatations (escape valves) will form in the non-visible perforating and communicating veins, where they will be more difficult to treat.
To treat varicose disease, we need to shrink the lumina and strengthen the walls of the veins. Moreover, since the entire venous circulation is a single network, treatment must not be limited to a localized area. A rational treatment for varicose disease therefore has to strengthen the walls and reduce the lumina of all the dilated and/or dilatable veins of the superficial and perforating circulation. Mechanistic treatments are not suited to biological material (even less so if its functioning is not fully understood).
Three-dimensional Regenerative Ambulatory Phlebotherapy (TRAP) treats the hemodynamic hypertension in the limb. The three-dimensional injection of the regenerative solution shrinks and strengthens the veins, restoring continence. Hence, the veins, venules and telangiectasias disappear from view.
Moreover, when the caliber of the veins is reduced, the blood flows more rapidly, improving the oxygenation of the patient.
In sum, the treatment of varicose disease must be seen in a holistic manner: the entire circulation is a single network; while hypertension is the same in all the vessels of the superficial circulation, those veins that have the weakest walls will become varicose; the veins should not be visible (when humans began to stand erect, the lower limbs became pumps, drawing blood from the superficial circulation into the deep circulation and pumping it towards the right atrium of the heart; a pump cannot work properly if it cannot draw liquid from the reservoir that supplies it – in this case, the superficial veins); once injected, the regenerative solution travels in the opposite direction to the formation of the varices; the saphenous vein is innocent; indeed, many individuals are born without valves in the saphenous vein, and yet they do not develop varicose disease; etc. (Concepts)
 |
|
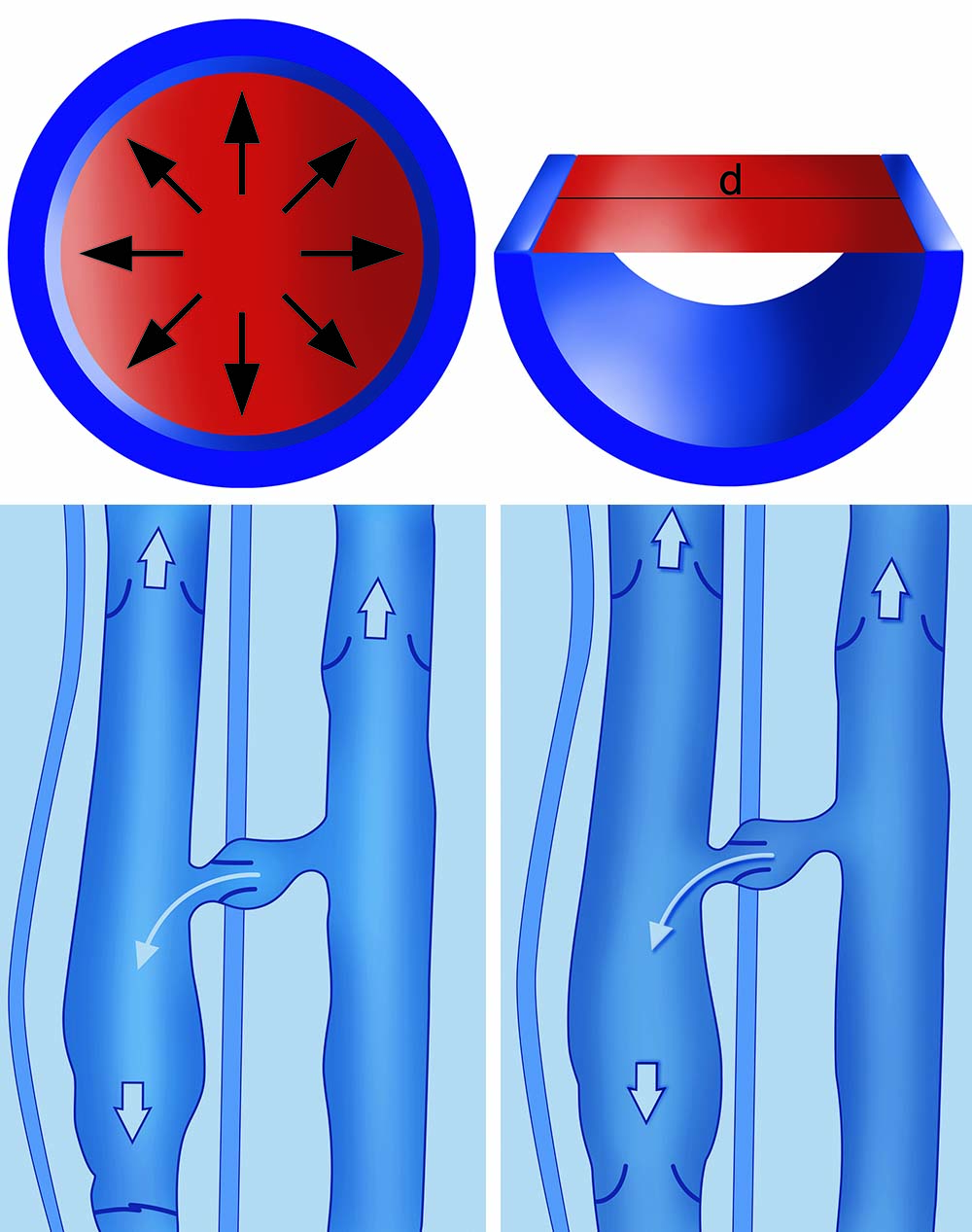
The underlying cause of varicose disease is meiopragia of the vessel walls, which is manifested by the dilation of the perforating veins. This leads to valvular incontinence, hemodynamic hypertension, dilation of the superficial circulation and a consequent increase in hydrostatic thrust (an absolute value, unlike transmural pressure). The first figure shows the onset of hemodynamic hypertension; the second illustrates the increase in hydrostatic thrust (hydrostatic pressure x the internal diameter of the vein x 1). |
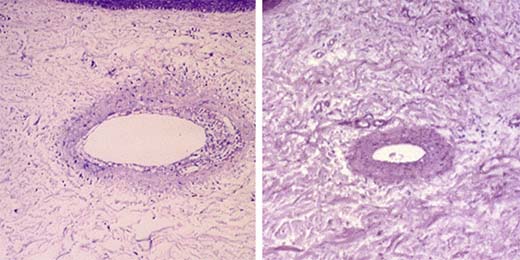
Regeneration Histology of venous wall (before and after)
 |
|
(Left) Histological section of skin (fixed in 10% buffered formalin, paraffin embedded and routinely processed; Weigert stain; enlargement 20 X). Dermal venule of medium-large calibre. The structure of this type of venule is characterised by sparse elastic fibres – not organised into a true, continuous elastic lamina – in the context of fibrous connective tissue of the wall. The vessel (visible “in vivo” as a phlebectasia) has a large eccentric lumen. The wall displays a non-uniform thickness and disorganised layers at several sites, and is permeated by a scant inflammatory infiltrate consisting mainly of lymphoid and monocytoid cells. The endothelial lining lacks continuity. Sub-endothelial microvacuolation is also seen. (Right) Histological section of skin. The same patient, the same area and a vein of equal size, seen after treatment with 6% sodium salicylate in an alkaline hydroglycerin buffered vehicle solution. Weigert stain; enlargement 20 X. The wall is of regular thickness. The internal endothelial layer is continuous. The wall shows no inflammatory infiltrate. Sodium salicylate in an alkaline hydroglycerin buffered vehicle solution treatment has restored uniform wall thickness, reduced the calibre of the lumen and consolidated the connective structure of the vessel wall. We have summarised these effects with the term “regeneration”. (Dr. Angela Sementa , Istituto Gaslini, Genova). |